I. IDENTIFICATION
Name(use initials when reporting for wider audience)
Age *
Occupation, Marital Status**
Religion
Address
* adolescents (< 18 ) and the elderly gravida (>35) are at
particular risk for adverse pregnancy outcome
**Information on marital status and occupation help assess the
socioeconomic status of the pregnant woman.
Low socioeconomic status is associated with several poor
pregnanacy outcomes Eg preterm labor, PROM, low birth
weight, anemia, Pre-eclampasia, Eclampsia 2
5.
II. chief complaints
Most pregnant women come for routine ANC
May have minor routine complaints
–eg abdominal discomfort, morning sickness,
back pain, leg pain, urinary frequency and
urgency,
Some complaints may mark a serious problem
/danger signs/ and warrant
–Eg- vaginal bleeding, ↓fetal movement,
headache, visual disturbance, leakage of liquor,
persistent vomiting ,sever abd’l/epigastric pain
3
6.
c/c………
Ex. Of Obst.C/Care:-
Vaginal bleeding
Leakage of liquor
Pushing down pain
Decreased/ absent FHB ?????
Absent fetal movement
Body swelling
headache, blurring of vision, etc.
• There may be more than one chief complaint.
• If more than one chief complaints are present,
they should be arranged in a chronological
order 4
7.
III. History ofPresent Pregnancy (HPP)
HPP is the most important part of obstetric
history and is composed of
1.Summary of reproductive performance
Gravidity
refers to all previous pregnancies i.e. term,
preterm, live birth, stillbirth, abortion, ectopic
pregnancy, molar pregnancy
Primigravidity (1st pregnancy) is associated with
increased risk of PIH, labor abnormalities, CPD and
obstructed labor
5
8.
• Ex. G3 means she had previous 2
pregnancies, now she is pregnant
for the 3rd time
6
9.
HPP
Parity
–all previous pregnanciesthat have reached
fetal viablity and delivered dead or alive
( i.e. >28 weeks of gestational age for
Ethiopia and UK , 28 weeks according to
other western countries)
–Primipara- 01 previous delivery
–Multipara- > 02 previous deliveries
–Grand multipara - > 5 previous deliveries
7
10.
Parity…..
Number ofbirths delivered after age of viability
(i.e. 28wks)
It could be live birth or still birth (born not alive)
Twin/triplet/ quadriplet etc
deliveries considered as one
parity.
Abortion-
Number of pregnancies terminated below the
age of viability, i.e <28 weeks
it could be induced or spontaneous.
Ectopic pregnancies:
– number of past extra uterine pregnancies, if there
was any. 8
11.
Examples
Ex. Thisis a 38 years old G 5, P 2, Ab1, Ectop 1
mother…… means,
she had 4 past pregnancies
o2 delivered
o1 aborted
o1 was ectopic pregnancy and
oshe is currently pregnant for the 5th time
9
12.
HPP……
2.Last normal menstrualPeriod (LNMP), EDD & GA
A.LNMP- 1st day of last menses
For LNMP to be reliable:-
1. It should be regular ( cycle length vary among
individuals ranging b/n 21 to 35 days)
2. It Should be similar to previous cycles in volume
and duration of flow
3. If the woman was on OCPs it should be
discontinued for at least 03 months ahead of
LMP
4. Lactating women should have 03 regular cycles
before LMP
10
13.
HPP……
B.EDD:-- 280 daysafter LMP= 40 weeks
EDD calculation;
1. Naegel’s Rule
– Subtract 03 months from LNMP and add 07days
– Eg If LNMP is February 12 then EDD will be on
November 19
2. Calculation according to the Ethiopian calendar
( 12 months of 30 days and pagume 5days/6
days with each leap year)
– LMP+ 9mths + 10days- if EDD doesn’t cross a year
– LMP+ 9mths + 5 days- if EDD crosses a year and
pagume is 05 days
– LMP + 09 mths + 04 days- if EDD crosses a year and
pagume is 6 days
11
14.
EXAMPLES
LNMP 10/1/07if EDD not cross the yr of NLMP
EDD will be on 20/10/07
LNMP 24/3/07 then EDD will be on 4/13/07
LNMP 30/3/01 if EDD cross the yr of NLMP;
EDD will be on 5/1/02
LNMP 6/6/01 then EDD will be on 11/3/02
12
15.
HPP…..
C. Gestational Age
•GA is calculated in completed weeks
– Preterm pregnancy:- GA < 37completed wks
– Early Term pregnancy:- 37 – 38 6/7 Week
– Full Term Pregnancy:- 39- 41 6/7
– Post-term pregnancy:- > 42 weeks
• GA calculation is based on the assumption a
28 day regular cycle length- ovulation on the
14th day
13
16.
HPP……
In additionto LMP other methods are used to estimate
GA
A. Early US before 20 weeks
– Ultrasonography may be considered to confirm menstrual
dates if there is a GA agreement
– within 1 week by CRL(crown ramp length) obtained in the
1stTM or
– within 10 days by an average of multiple fetal biometric
measurements (eg, CRL, BPD, HC, AC,FL) obtained in the
2nd (up to 20 weeks GA) . ACOG-2008
B. Quakening date
– around the 17th week for multipara ( experience from
previous pregnancies)
– Around the 19th week for primipara
C. Fundal height at umbilicus~20 weeks, 12 wks at
symphysis pubis and 38 wks at xiphysternem. 14
17.
HPP…..
3.ANC hx
• Ifno ANC or delayed state – reason
• Details of ANC
– when, where started?
– what was done during each visits?
• What type counseling, examination
• investigation, medications given?
– Pre-pregnancy weight /BMI and weight at booking and on subsequent
visits
– BP recordings
– Lab investigation results
• Blood group, Rh, hemoglobin level
• UA for bacteruria, infection and hCG
• RVI,
• RPR/ VDRL test
• HBsAg 15
18.
HPP/ANC……
• Health educationabout nutrition, sanitation,
labor, breast feeding and contraception
• Iron supplementation, malaria prophylaxis, TT
immunization,
• Any drug use- prescription, over-the-counter
or herbal medications
• Significant symptoms of illness early in
pregnancy like excessive nausea and vomiting,
Vaginal bleeding
16
19.
HPP…..
4. Detailed discussionof the presenting
complaint (C/C) /xziation of symptom/
5. Always ask about the common danger signs
of pregnancy
– Headache (severe, persistent, not responsive for
analgesia)
– Visual disturbance
– Epigastric/ RUQ pain
– Vaginal bleeding
– Leakage of liquor per vagina
– Fetal movement status 17
20.
HPP
6. Positive andnegative statements directed at
possible DDx to the presenting complaint
7. Relevant informations should be switched
from other sections ( past ob Hx, Medical and
surgical hx , family hx etc. ) to the HPP.
8. Pregnancy;
– unplanned , unwanted and unsupported
18
21.
IV. Nutritional Hx
•Detailed enquiry whether the woman takes
adequate amount of carbohydrates, fat,
proteins , minerals and vitamins
• Look for any food restrictions for cultural
reasons or taboos
19
22.
V. Past ObstetricHistory
• Detailed chronological documentation of all
previous pregnancies i.e.
– Date , month and year of gestation ,
– gestation length (weather abortion , PT, term,post
term)
• Any antepartum, intrapartum or postpartum
complications
– Eg APH, PPH, IUGR, PROM, Malpresentation,
macrosomia, congenital anomalies, molar pregnancy,
GDM, Hypertensive disorder
NB- most of these complications have a significant
recurrence risk
20
23.
• Onset oflabor (spontaneous or induced
• Fetal presentation
• Duration of labor
• Mode of delivery (SVD , instrumental, C/S,
destructive delivery
• Fetal outcome (alive or dead, sex of the
newborn, weight of the newborn
malformations, current condition)
21
24.
VI. Gynecologic History
•Menstrual history
– Age at menarchae
– Regular/ irregular, intervals (21-35 days ),intermenstrual
bleeding/ spotting
– Amount and duration of flow
– Discomfort during menses (Dysmenorrhoea)
– Premenstrual symptoms (cyclic affective and somatic
symptoms in the luteal phase)
• Contraception use history
– use , type , duration and side effects
22
25.
• Sexual history
–assessrisk of sexually transmitted
infections and HIV/AIDS
• Gynecology operations
–Female genital mutilation
–laparatomy,
–dilatation and curettage ,
–Evacuation and curettage,
–manual vacuum aspiration
23
26.
VII. Past medicaland surgical History
• Episodes of acute/ chronic illnesses, duration,
treatment outcome , follow up , current status
• Such chronic illnesses as DM, HTN, Thyroid
disease ( thyrotoxicosis and hypothyroidism),
cardiac and renal disease that affect pregnancy
outcome need to be integrated with the HPP
• Hx of blood transfusion-
– possibility of minor blood group incompatibility and Rh
isoimmunization
• STI Hx and treatment
• Hx of pelvic surgery
– Eg –myomectomy, hysterectomy, metroplasty- cause uterine
scarring and may dehisce during pregnancy and labor
• Hx of surgery involving other organ systems
24
27.
VIII.Personal and FamilyHistory
• Place of birth and bringing up
• Education, occupation, income
• Habit of smoking, alcohol , caffein or illicit drug use
• siblings-
– Number of sisters and brothers
– Alive
– Dead – cause of death
• Parents
– Age
– Health status
– If deceased- age when dying and cause of death
• Family history of chronic illnesses ( eg DM,
Hypertension Epilepsy etc.) or any hereditary disease
• Family history of twining
25
28.
IX. Review ofSystem (Functional enquiry)
• Detailed orderly search for any symptoms
pertaining to each organ system LIKE medical
history
• Gus Hx & danger signs like headache and
blurring of vision are put in the HPP.
26
29.
Physical Examination
1. GeneralAppearance
– Comfortable, in CRD, acutely/ chronically sick
looking,
– body habitus ( obese, malnourished), stature
(extremely short?), skeletal deformities
– Facial features- chloasma of pregnancy, puffy
face
NB. some of the above descriptions can be
placed at the respective systemic examinations
27
30.
2. Vital Signs
BP
– Measured in the left lateral ( usually for
inpatients) or sitting positions
– The right arm should be used consistently, in a
roughly horizontal position at heart level.
– For DBP, both phases ( IV-muffling and V-
disappearance of sound) should be recorded.
PR, RR, T0
– are taken the same way as in any medical patient
physiologic changes caused by pregnancy should be taken
into account while interpreting results 28
31.
3. HEENT
– lookfor chloasma, Conjunctival pallor /PINK, icteric /jaundiced
sclera
– Hair distribution
– Buccal mucosa- wet or dry ?
– Gingival hypertrophy, gingivitis?
– Oral thrush?
4. LGS-
– Breast (engorgement, areolar pigmentation ,montgomery tubercles….),
thyroid and all accessible LN areas are examined
5. Chest
– Inspection, palpation, percussion and auscultation of RS.
6. CVS
– PMI displacement lateral to the MCL, S3 and systolic murmurs <
Grade III are usual non pathologic findings
– Look for varicose veins in the lower extremities and vulva -(DVT)
29
32.
7. Abdomen
• Exposure
–The patient should be supine with a comfortable
pillow, the arms lie by her sides
– The abdomen should be exposed from just below
breasts to the symphysis pubis just below the pubic
hairline ( not to miss pfannenstel scar)
NB- the woman is often asked to expose the
abdomen by herself
30
33.
Inspection
• Grossly distendedabdomen?
• Protuberance- central or localized tone area
• Movement of abdomen with respiration
• Flank fullness
• Uterine dextrorotation ( abdomen tilted more to the right normally in px
women bcz of sigmoid on the left side)
• Black line (linea nigra) more prominent in the midline b/n umbilicus and and
symphysis pubis.
• Striae gravidarum- stretch marks due to disruption of collagen fibers of
dermis ( breasts and thighs can also be involved)
– NEW- purplish, few
– Old (straie albicantes)- whitish, multiple
• Umbilicus-flat, inverted, everted?
• Scar- location, size and thickness
• Distended veins and ascites portal hypertension
• Abdominal wall edema with peau-d-orange appearance part of ana sarca
31
34.
Superficial palpation
• Ineach quadrant
– areas of rigidity, tenderness, abd wall masses
– Location of appendix base in advanced
pregnancies at higher level than McBurneys point
( pushed up by the gravid uterus)
– Diffuse tenderness and rigidity /generalized
peritonitis:--
»chorioamnionitis
»abruptio placentae,
»ruptured appendicitis,
»perforated PUD
32
Obstetric Palpations (Leopold’smaneuvers)
• Four sequential maneuvers Performed on the
gravid uterus i.e. the fundal, lateral, pelvic
palpations and the Pawlik’s grip.
NB:-
• Before 28 weeks of gestation fundal height
determination is the only palpation possible
as the fetus is too small to determine lie or
presentation
• Fetal heart beat can be auscultated from 20th
week of gestation
34
37.
1- Fundal Palpation
Objectives:-
•Determination of Height of fundus-GA and what
occupies the fundus
• Abdominal asymmetry need to be corrected first
( if dextro or levorotation is there) and the
bladder should be empty before starting
examination
A. Fundal Height determination; two methods i.e;
– Tape measurement of symphysis fundal hgt (SFH) in
cms or
– Finger method
35
38.
1. SFH TapeMeasurement (Tape Measurement)
–In the midline along the linea nigra traversing
the umbilicus
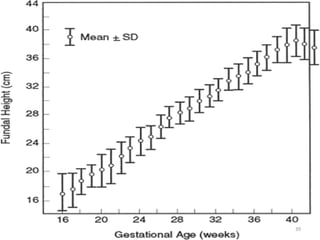
–The fundal height in cm accurately matches
to the gestational age b/n 18- 34 weeks
–More reliable method than the finger method
36
39.
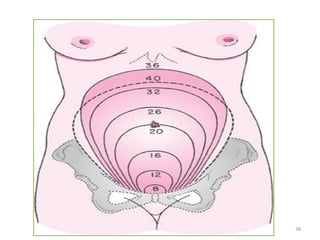
2. Finger method
–Fundusjust palpable at S.pubis 12 weeks
–Midway b/n S.pubis and umbilicus 16 wks
–At Umbilicus 20 weeks
–Generally 1 finger above umbilicus
represents 2 weeks
–At Xiphysternem 38 weeks/term
–36 week by finger is comparable to 40
weeks of GA due to decrease in fundal
height after engagement
37
NB:--
A fundalheight to GA discrepancy of up to 02
weeks is acceptable.
A positive or negative discrepancy of more than 02
week mandates further investigation to identify the
possible underlying cause.
The commonest cause of both +ve and –ve
discrepancies (large for date and small for date
respectively) is wrong dating.
Other possible causes
+ve Discrepancy multiple gestation, polyhydramnios,
macrosomia, GTD, leiomyoma, ovarian tumor,
-ve discripancy IUGR, oligohydramnios, PROM,
transverse lie, IUFD, missed abortion
40
43.
B. Determining WhatOccupies The Fundus
• Palpate and ballot the fundal area with
both hands
–Head hard, round, ballotable structure
–Breech soft, bulky, irregular, non
ballotable
41
44.
2- Lateral Palpation
Objective:-
Determination of fetal lie and identification of the
side of the back
1. Fetal lie
– Orientation of the fetal longitudinal axis with respect
to that of the mother i.E longitudinal, transverse or
oblique
– Lateral palpation is performed alternatively on both
sides using one hand to stabilize the uterus.
2. The back feels like hard, straight/ flat structure
while the extremities on the opposite side feel
like multiple nodular parts
– Fetal heart beat can be easily auscultated on the side
of the back
42
45.
3.pelvic palpation
Objectives
• identificationof fetal presentation and attitude ( if
cephalic) Cephalic prominence
• The examiner faces the patient's feet and places a hand
on either side of the uterus, just above the pelvic inlet.
• When pressure is exerted in the direction of the inlet,
one hand can descend farther than the other.
• The part of the fetus that prevents the deep descent of
one hand is called the cephalic prominence.
• Presentation can be Cephalic , breech or shoulder
43
46.
Attitude
– Flexed;the cephalic prominence is on the same
side as the small parts.
– Extended; the cephalic prominence is on the same
side as the back.
– military
Descent=from 5/5 ( floating) to 0/5
Engagement=minimum of 2/5 descent
44
47.
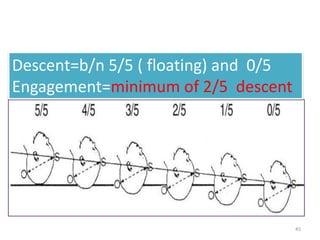
Descent=b/n 5/5 (floating) and 0/5
Engagement=minimum of 2/5 descent
45
48.
4.Pawlik’s Grip
Objective-
Identificationwhat fetal part lies in the lower segment
( presentation) and its mobility
A single examining hand is placed just above the
symphysis.
The fetal part that overrides the symphysis is grasped
between the thumb and third finger.
If the head is unengaged, it is readily recognized as a
round, hard object that frequently can be displaced
upward.
After engagement, the back of the head or a shoulder
is felt as a relatively fixed, knoblike part.
In breech presentations, the irregular, nodular breech
is felt in direct continuity with the fetal back
46
49.
Abdominal FindingsIn Multiple Gestation
–multiple fetal poles
–2 FHRs at 2 sites , a difference of > 10 bpm,
FHR auscultated simultaneously by two
examiners i.e for twin pregnancy
47
50.
PE- GUS
Inspection
• Lookfor Normal development of the external genitals
(The Vulva)
– Mons pubis (Veneris), Labia majora and minora, urethra, Skene
(paraurethral) Glands,Vestibule, Bartholins (Great vestibular)
glands, The Hymen, Fossa Navicularis
• Hair distribution-
– Normal findings
• Inverted triangle pattern with a base over the Mons Pubis.
• The labia majora are also covered
– Extension of hair to the abdomen is abnormal for females
( Hirsutism)
• Look for skin lesions ( warts), discharge (vaginal or
urethral),Scars, Swelling and Prolapse ( descent with or
without exertion)
48
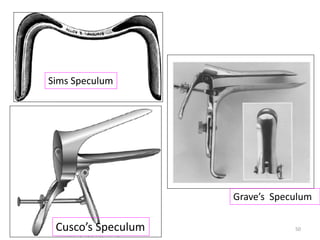
Speculum Examination
•Position; dorso lithotomy
• Warm and lubricate the speculum (clean
speculum for most gynecologic examinations)
• Insert the speculum with the transverse
diameter of the blades anteroposteriorly and
guide the blades through the introitus in a
downward motion with the tips pointing toward
the rectum
• Then turn the blades so that their transverse axis
is along with the transverse axis of the vagina
• Open the blades after full length insertion of the
speculum the cervix should be visible b/n the
blades
51
54.
Speculum Examination
Inspectthe vagina and Cervix
• Vagina
– Discharge , inflammation (erythema), Mass (e.g
Gartner's cyst)
• Cervix
– External OS ( shape, discharge from), SCJ, Nabothian
cysts, Lesions (polyp, ulceration, nodularity,
inflammation), bleeding
– Cervical Ca screening ( Cytology via Pap smear or visual
methods via VIA / VILA) can be performed if indicated
and possible.
– Discharge specimen is taken for wet mount and KOH test
52
55.
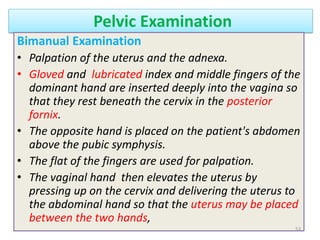
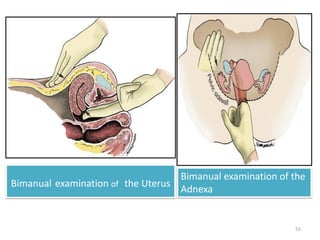
Pelvic Examination
Bimanual Examination
•Palpation of the uterus and the adnexa.
• Gloved and lubricated index and middle fingers of the
dominant hand are inserted deeply into the vagina so
that they rest beneath the cervix in the posterior
fornix.
• The opposite hand is placed on the patient's abdomen
above the pubic symphysis.
• The flat of the fingers are used for palpation.
• The vaginal hand then elevates the uterus by
pressing up on the cervix and delivering the uterus to
the abdominal hand so that the uterus may be placed
between the two hands,
53
56.
• Both adnexaare also examined in the same
way through the lateral fornices
• Bimanual Examination helps identify
– Position ( often anteverted and anteflexed) , size,
shape, consistency, and mobility of the uterus
– Whether the adnexa are papable or not
– The presence or absence of uterine or adnexal
masses
54
Notice the followingwhile performing Bimanual
Exam
ሀ .Cervix
• Excitation / motion tenderness
– Move the cervix gently to each side with one finger.
– Pain points at a tuboovarian mass (ectopic, abscess)
or inflammation.
• Consistency
– A normal cervix is firm (tip of nose) but not hard,
– In pregnancy it is softer with a firmer core.
– In cervical cancer the cervix can be hard, broad, with
an irregular surface.
56
59.
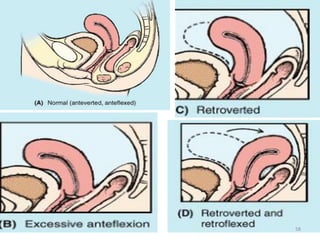
ለ.Uterus
• Axis/ position
–Anteverted--anteflexed (most common), retroverted or
straight
• Size
– Enlarged size pregnancy, leiomyoma, sarcoma etc
– A large tubo-ovarian mass can be mistaken for an
enlarged uterus.
– Uterine mass moves with the cervix but not adnexal
masses
• Consistency
– Normally firm , A gravid uterus is soft, uterine fibroids are
hard or at least firm; advanced uterine or cervical
malignancy is often hard but endometrium carcinoma
can present as a soft enlarged uterus as well.
57
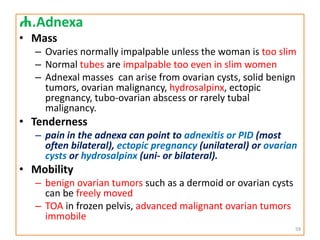
ሐ.Adnexa
• Mass
– Ovariesnormally impalpable unless the woman is too slim
– Normal tubes are impalpable too even in slim women
– Adnexal masses can arise from ovarian cysts, solid benign
tumors, ovarian malignancy, hydrosalpinx, ectopic
pregnancy, tubo-ovarian abscess or rarely tubal
malignancy.
• Tenderness
– pain in the adnexa can point to adnexitis or PID (most
often bilateral), ectopic pregnancy (unilateral) or ovarian
cysts or hydrosalpinx (uni- or bilateral).
• Mobility
– benign ovarian tumors such as a dermoid or ovarian cysts
can be freely moved
– TOA in frozen pelvis, advanced malignant ovarian tumors
immobile
59
62.
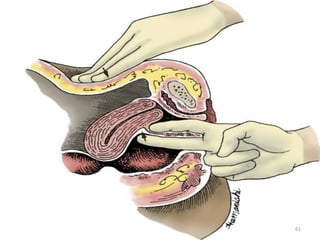
Rectovaginal examination
• Therectovaginal palpation is not necessary in
every patient
• Often done in cases when there is suspicion of
malignancy, endometriosis or any process located
in the pouch of Douglas.
• It helps to assess the structures between the
vagina and rectum.
– Eg Rectovaginal septum, Uterosacral ligaments
• Mass, thickening, tenderness of these structures
may be caused by malignancy, inflammation or
endometriosis
• Retroverted uterus can also be examined ( size,
shape, consistency) through the RV route
60
Rectal Examination
• Invirgins, a vaginal examination is avoided.
• Instead a well-lubricated finger inserted into the
rectum can be used for a bimanual assessment of the
pelvic structures.
• Today, practically all gynecologists prefer ultrasonic
scanning to rectal examination, which, apart from
being unpleasant, is not that accurate.
• A rectal examination is a very useful additional
examination whenever there is any palpable pathology
in the pouch of Douglas.
• It often allows the ovaries to be more easily identified.
• In parametritis and endometriosis, the uterosacral
ligaments are often thickened, nodular and tender.
62
65.
• It confirmsthe swelling to be anterior to the rectum,
and if the rectum is adherent to that swelling.
• This is important in case of carcinoma of the cervix to
determine the extent of its posterior spread.
• A rectal examination is mandatory in women having
rectal symptoms.
• This should begin by inspecting the anus in a good
light, when lesions like fissures, fistula-in-ano, polyps
and piles may come to light.
• Introduction of a well-lubricated proctoscope to
inspect the rectum and anal canal helps to complete
the examination.
• Ultrasound today has reduced the importance of rectal
examination except in cancer cervix and pelvic
endometriosis.
63
Follicular Development
• Folliculardevelopment begins with primordial follicles
that were generated during fetal life
• Primordial germ cells can be identified in the yolk sac
as early as the third week of gestation
• These cells begin their migration into the gonadal ridge
during the sixth week of gestation
• In the gonadal ridge the primordial cells undergo
successive mitotic divisions and produce the OOggonia
• Starting at 12 weeks’ gestation, a subset of oogonia will
enter meiosis –which is arrested at prophase I –and
become primary oocytes .
• primordial follicles are formed by surrounding Primary
oocytes are surrounded by a single layer of flattened
granulosa cells
70.
Follicular Development
Primordial Follicles
–20th wk of GA- 6-7 million
– Birth- 1-2 million Primordial Follicles (additional
oocytes cannot be generated postnatally)
– Puberty ~ 400,000 (< 500 are ovulated)
– < 1,000 follicles at the onset of menopause
• Only 400 follicles are normally released during
female reproductive life.
> 99.9 % of follicles undergo atresia through
apoptosis
• Rate of follicular atresia
– 1000Fs/month (until age 35)
– Faster rate at > 35yrs
71.
• Primordial Follicle
10 oocyte ( arrested at Prophase I)
surrounded by single layer of flat Granulosa
cells
72.
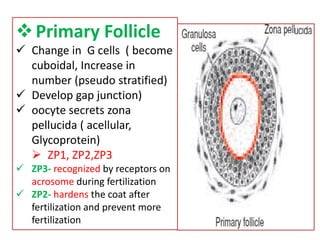
Primary Follicle
Changein G cells ( become
cuboidal, Increase in
number (pseudo stratified)
Develop gap junction)
oocyte secrets zona
pellucida ( acellular,
Glycoprotein)
ZP1, ZP2,ZP3
ZP3- recognized by receptors on
acrosome during fertilization
ZP2- hardens the coat after
fertilization and prevent more
fertilization
73.
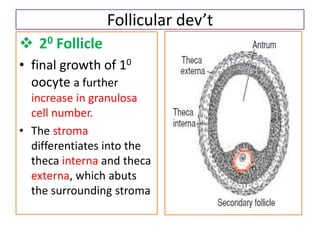
Follicular dev’t
20Follicle
• final growth of 10
oocyte a further
increase in granulosa
cell number.
• The stroma
differentiates into the
theca interna and theca
externa, which abuts
the surrounding stroma
74.
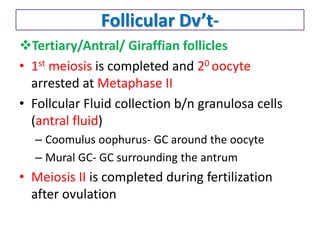
Follicular Dv’t-
Tertiary/Antral/ Giraffianfollicles
• 1st meiosis is completed and 20 oocyte
arrested at Metaphase II
• Follcular Fluid collection b/n granulosa cells
(antral fluid)
– Coomulus oophurus- GC around the oocyte
– Mural GC- GC surrounding the antrum
• Meiosis II is completed during fertilization
after ovulation
75.
Follicular Development
• StagesFrom Recruitment of Primordian
follicle (from the resting pool) to preantral
stage are Gtropin Independent stages, but
beyond this stage FSH is required and the follicles
undergo atresia if no FSH
• Follicular atresia since the fetal age
• Late Luteal Phase- Small rise in FSH
semisynchronous growth of Cohort of Antral
follicles
• Dominant Follicle
– the one most responsive for FSH increased E
and InhibinB decline in FSH failure of other
follicles to reach the preovulatory stage
Spermatogenesis
• Takes placein the seminiferous tubules of
testes
• The germinal epithelium cells undergo
continuous mitosis and enter meiosis
• Maturation period of spermatozoa~ 70 days
78.
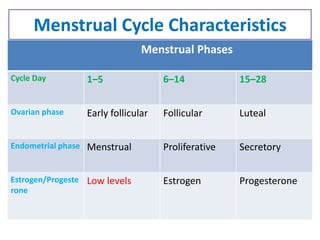
Menstrual Cycle
Ovarian andEndometrial components
1. Ovarian Cycle- two phases
– Follicular phase (Preovulatory)
• From onset of menses to just before ovulation
• Time for recruitment of cohort follicles and growth
and maturation of the dominant follicle among the
cohort
– Luteal phase (Postovulatory)
• From ovulation till the next menses
• Corpus luteum formation, both granulosa and
luteal cells produce progesterone.
• Relatively constant duration (lasts app for 13- 14
days)
79.
2. Endometrial cycle
•Proliferative Phase
– Corresponds to the follicular ovarian phase ( usually from 6th
to 14th day)
– Endometrial glandular cells proliferate, mainly under
estrogenic influence
– Tubular Glands and straight arterioles, edematous stroma
• Secretory Phase
– Correspond with luteal phase
– Glands become tortous and with subnuclear vacuoles that
secret glycogen rich material into the lumen
– Vessels become coiled
– Mainly due to influence of progestrone
Ovulation and Fertilization
•Ovulation the process by which the oocyte
cumulus is released from the follicle
• The oocyte-cumulus complex is then picked/
engulfed immediately by infindibulum of the
oviduct and infundibulum.
• Further transport through the tube is
accomplished by directional movement of
cilia and Tubal Peristalsis.
• Ovulation is preceded by LH surge 18-36 hrs
ahead
83.
Ovulation and Fertilization
•Union of sperm and egg takes place in the
fallopian tube( site of fertilization)
• Life span of egg ~ 24hrs and that of Sperm ~ 5
days
• Window of fertilization 3days per cycle
– i.e the day of ovulation and the 2 preceding days
84.
Ovulation and Fertilization
•Spermatozoa matures in 72 days since onset of
spermatogenesis reaches caudal epididymis
and is ready for ejaculation
• During coitus sperm cells enter cervical mucus
and swim upwards to the uterine cavity and then
to Fallopian Tubes
• The cx mucus forms linear alignment parallel
strands that guide the sperms upward
• Sperm movement is also assisted by uterine
contraction
85.
Ovulation and Fertilization
•The cervical mucus also serves as sperm
reservoir for ~ 72hrs and medium of
capacitation of the sperm.
• Capacitation- the process which makes the
sperm capable of penetrating the ova
– Occurs in the female genital tract ( Cx and FTs)
• Capacitation of the sperm results in;
1. The ability to undergo the acrosome reaction.
2. The ability to bind to the zona pellucida.
3. The acquisition of hypermotility.
87.
Ovulation and Fertilization
•Fertlization involves highly complex steps of
molecular activities so that the spermatozoa
can
– Pass the cumulus cells and zona pelucida (thick
glycoprotein overlying the Oocyte cell membrane)
– Penetrate and end enter into the oocyte
cytoplasm and effect Fusion of the two nuclei.
• intermingling of maternal and paternal
chromosomes creates the zygote.
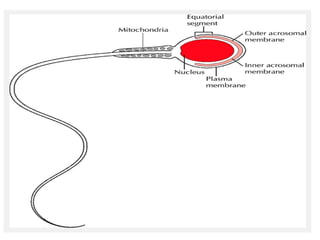
88.
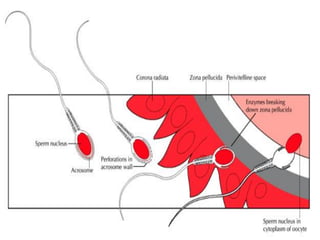
Steps in Fertilization
•Sperm passes through the cumulus ,binds to zona ligands
and Penetrates ZP
• Binding of sperm head receptors and zona ligands induces
Acrosome Reaction, releasing enzymes essential for the
fusion of the sperm and oocyte membranes.
• Following sperm and oocyte fusion the cortical reaction
leading To Zona Reaction hardens the ZP and prevent more
sperm penetration.
• The cortical reaction leads to the enzyme-induced:-
– zona reaction, the hardening of the zona and
– the inactivation of ligands for sperm receptors, producing an obstacle
to polyspermy.
• Cell division begins promptly after fertilization; human gene
expression begins between the 4- and 8-cell stages.
90.
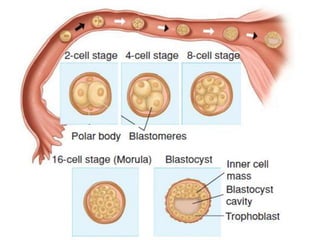
The Zygote
• Thezygote—a diploid cell with 46 chromosomes
which results from fertilization
• The zygote undergoes slow cleavage for 3 days in the
Fallopian Tubes
• The cells produced by this division are called
Blastomeres.
• As the blastomeres continue to divide, a solid
mulberry-like ball of cells— the Morula —is produced.
• The morula enters the uterine cavity about 3 days after
fertilization
• Gradual accumulation of fluid between the morula
cells leads to formation of the early blastocyst.
Zygote blastomers morula blastocyst
92.
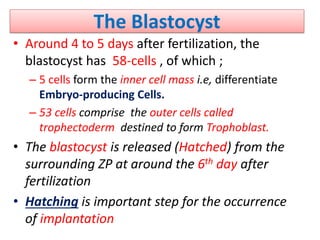
The Blastocyst
• Around4 to 5 days after fertilization, the
blastocyst has 58-cells , of which ;
– 5 cells form the inner cell mass i.e, differentiate
Embryo-producing Cells.
– 53 cells comprise the outer cells called
trophectoderm destined to form Trophoblast.
• The blastocyst is released (Hatched) from the
surrounding ZP at around the 6th day after
fertilization
• Hatching is important step for the occurrence
of implantation
93.
Blastocyst Implantation
• 6or 7 days after fertilization, the embryo implants
in the uterine wall.
• uterine receptivity is limited to days 20 to 24 of
the cycle window of implantation
The Implantation process has 3 phases:
1. Apposition— initial contact of the blastocyst to
the uterine wall;
2. Adhesion— increased physical contact between
the blastocyst and uterine epithelium; and
3. Invasion— penetration and invasion of
syncytiotrophoblast and cytotrophoblasts into
the endometrium, inner third of the
myometrium, and uterine vasculature.
96.
Implantation
• After gentleerosion between epithelial cells of
the surface endometrium, invading trophoblasts
burrow deeper.
• By the 10th day, the blastocyst becomes totally
encased within the endometrium.
• The mechanisms leading to Trophoblast invasion
are similar to those of metastasizing malignant
cells
97.
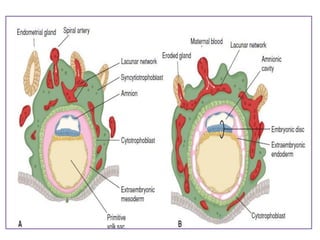
Implantation
• Embryonic mesenchymefirst appears as isolated
cells within the blastocyst cavity.
• When the cavity is completely lined with this
mesoderm, it is termed the chorionic vesicle, and
its membrane, now called the chorion, is
composed of trophoblasts and mesenchyme.
• Some mesenchymal cells eventually will
condense to form the body stalk.
• This stalk joins the embryo to the nutrient
chorion and later develops into the umbilical
cord.
• The body stalk can be recognized at an early stage
at the caudal end of the embryonic disc
98.
Implantation
The Decidua;
• specializedendometrium of pregnancy
• Decidua Basalis:-directly beneath the
implanting blastocyst- 3 layers Compact,
spongy and basal
• Decidua Capsularis covers the upper
portion of the blastocyst.
• Decidua Parietalis the rest
• With obliteration of uterine cavity D. Capsularies and
D. Parietalis merge and form D. Vera
99.
Trophoblasts
• Human placentalformation begins with the
trophectoderm, which appears at the morula and
blastula stage.
• It gives rise to a Trophoblast cell layer encircling the
blastocyst.
• From then until term, the Trophoblast plays a critical
part at the fetal-maternal interface.
• Trophoblast exhibits the most variable structure,
function, and developmental pattern of all placental
components.
• Its invasiveness promotes implantation, its nutritional
role for the conceptus is reflected in its name, and
• its endocrine organ function is essential to maternal
physiological adaptations and to pregnancy
maintenance.
100.
Trophoblasts
• By the8th day post-fertilization, after initial
implantation, the Trophoblast has differentiated
into;
1. Syncytiotrophoblast - an outer multinucleated
primitive syncytium;
– has an amorphous cytoplasm without cell borders,
multiple nuclei that are diverse in size and shape,
and a continuous syncytial lining.
– This configuration aids transport.
2. Cytotrophoblast- an inner layer of primitive
mononuclear cells— are germinal cells for the
syncytium.
– Contrary to syncytiotrophoblast ,each cytotrophoblast
has a well-demarcated cell border, a single nucleus,
and ability to undergo DNA synthesis and mitosis